It’s been a busy few weeks for us at Endeavor as almost all of our players are back at this point. It’s been a fun off-season already, as we’ve had a couple special situations of early arrivals, short-term training availability, combine prep, etc. I’ve been more stringent in re-assessing and tracking various qualities as time goes by so it’s been interesting to see how our players respond/progress through the various phases. A few random thoughts that have come up the last few weeks:
It’s been neat to see how some players resting heart rate and heart rate variability shift dramatically toward more ideal levels after a 3-4 week aerobic oriented phase, and how some players have gained ~15 degrees of rotation arc in their hips after 3-4 weeks, presumably because of the corrective work we’ve prescribed. I talked a little more about some of the other early results we’ve seen with some of our off-season programs in a previous post: Off-Season Hockey Training Programs
It’s always nice to have evidence that players are adapting in the direction you want, but it’s also valuable to learn when players are NOT adapting, which allows a deeper thought process as to what may be limiting the adaptation. For example, many of our players continue to have limited ankle mobility, despite putting a strong focus on improving dorsiflexion ROM across several weeks. For some players, it’s definitely a tracking issue and some targeted soft-tissue work and different mobilizations may do the trick. For others, I strongly believe they have a structural deviation of the ankle mortice that limits this ROM, similar to how FAI limits hip flexion ROM. For more information on ankle mobility, check out these two old (but still very current) articles from Carson Boddicker: Alleviating Ailing Ankles, Alleviating Ailing Ankles II
I got an email from a parent of a 9-year old wondering why his son plays with such an observable drive during practice, but seems much more timid in games. This is something I imagine many parents with young athletes in all sports wonder. The first thing that comes to mind is that the player is 9, and it really doesn’t matter, as long as he’s having fun. The second thing, which is very related, is that the player is likely performing at a higher level in practice because he feels free to play and try new things without the pressures of in-game consequence. If you try a new move and fail in practice, it doesn’t matter; no one is keeping score. In fact, that is the point of practice. In a game, especially in the win-at-most-costs culture we’ve created for our youth athletes, the stakes are much higher and the player is probably thinking (consciously or subconsciously) that it’s better to avoid making mistakes than the potential reward of succeeding at something more risky. This really highlights the importance of rewarding behavior, and not outcomes. Encourage kids to be creative AND to make mistakes. No one cares if you win when you’re 9.
Today alone, we had two examples of HRV values showing “red flags” that have allowed us to alter our programming to allow a player to recover better. One case was related to too much fun over the weekend; the other simply needed a longer recovery period from a previous phase. In both cases, the player completely understood why we needed to change things and values the fact that we’re individualizing things to allow for the most optimal adaptation. I’m working on ways to build HRV monitoring into the programs of all of our 4-day/week players, as I strongly believe that this simple measure provides a powerful indicator of the individual’s current adaptation capacity, and the state of their autonomic nervous system. If you’re unfamiliar with HRV, I’d encourage you to read this post: BioForce Heart Rate Variability
Because I’ve written a lot about Femoroacetabular Impingement (FAI) and have worked with number of athletes that were surgical candidates, were post-surgery, or are in an “at-risk” population, I get emails almost weekly from people suffering from FAI symptoms that are looking for advice. While I think it can be valuable to do some reading online to better understand what may be driving your dysfunction, it’s EXTREMELY difficult to self-treat injuries, especially those involving structural changes. It’s equally difficult to diagnose injuries over the internet. I can’t understate the importance/value of seeking out a quality health care professional for a thorough assessment. I work closely with a few guys in our area that we send athletes to regularly when I need another set of eyes or if they require manual/treatment skills that I don’t possess. If you’re a S&C professional, build a network of physical therapists, chiropractors, and functional medicine/osteopath/naturopath physicians in your area. Not only can they be a good source of referrals, but sending a client to the right professional at the right time is a great way to stimulate more word of mouth marketing. For everyone else, the same mentality is still valuable; build a healthcare team in your area. It’s the best way to manage your own health and performance.
I have a lot of other random thoughts floating around my head, but our afternoon groups are starting and I have a couple players to assess! Until next time…
Please enter your first name and email below to sign up for my FREE Athletic Development and Hockey Training Newsletter!
Breakaway Hockey Speed Q&A
The other day I got an email from a hockey dad that had just downloaded and started diving into Breakaway Hockey Speed, and immediately had some questions. Based on what he told me, he has two sons that have completely different skating styles (which is something I discuss in the manual), and was hoping to get some clarification on “ideal” skating patterns.
He wrote:
Kevin, I signed up for Breakaway Hockey Speed and am reading it now.It’s awesome! It rings very true to me. You don’t look like a very old guy but the observations here would seem to have taken a lot of time or some very careful observation over a number of years.
The reason it rings true to me is that I played hockey all my life and now have two boys ages 12 and 10 who have played since they were old enough to skate. And the two have totally different skating styles.
It’s been a real nature vs. nuture observation for me – they both learned the exact same way and they both did the exact same programs. But they have two very different body types (youngest one lean and flexible, the older more dense with a more limited range of motion) and that certainly seems to have been the biggest difference in their development as hockey players and skaters.
I’ve cut out parts of the message, but his questions and my responses are below:
1) How does one determine their optimal skating depth based on their individual build and joint range of motion (ROM)? Should working on improving ROM be the priority instead of adapting to a sub-optimal situation?
Skating depth based on an individual’s build goes much deeper than muscle flexibility. The contour of the hip joint itself and the length of the femurs relative to the torso will both play a huge role where a player’s optimal body position falls. Longer femurs relative to a shorter torso (this can occur in tall and short people as it’s the ratio, not the absolute lengths that’s important) will necessitate that the player maintains more of a forward torso lean to position his or her center of gravity appropriately above their skates. This will necessitate more hip flexion range of motion, which the individual may or may not have, or will result in a spinal flexion (rounding, particularly of the lower back) which is likely to cause discomfort in this area over time. Allowing this player to skate “higher” than some arbitrary “norm” isn’t allowing them to adapt to a sub-optimal situation, it’s keeping them out of sub-optimal positions altogether. I’m sure these things could all be measured, but that’s really not necessary. You just need to have a good eye for how they move.
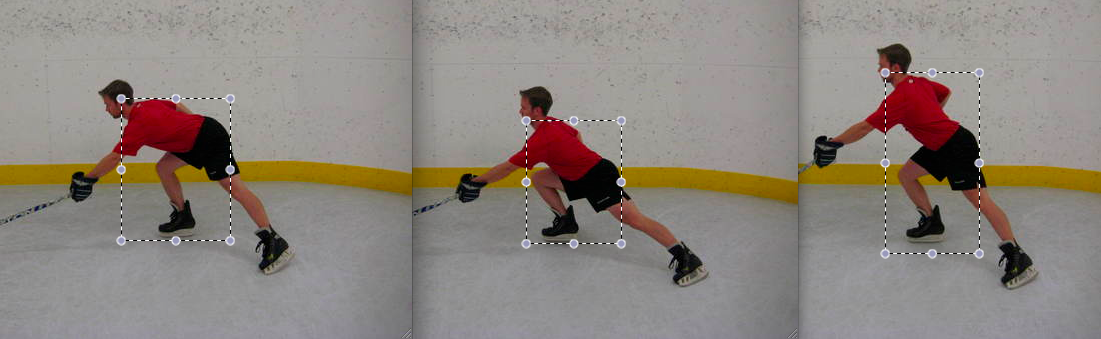
In reality, the “ideal” stride is almost the same for everyone: it’s the lowest depth that a player can achieve keeping their hips above their knees, maintaining a neutral spine with their center of gravity balanced appropriately over the skates. In Ultimate Hockey Training, I’ve included some pictures of extreme situations to help illustrate how “lower” is not always better.
In this picture, the degree of hip flexion (think torso lean) is way too far. Note that I still have a fairly neutral lumbar spine (lower back) in the picture, which is desirable. However, the angle of torso lean is such that it unloads the stride leg, so it’s not possible to produce as much propulsive force off that leg.
In this picture, the degree of knee flexion is way too far. This shifts the COG too far behind the lead leg, but the deep bend also makes roughly the first half of the stride very awkward, as it’s essentially just repositioning behind the COG to be able to create propulsive force.
In contrast to the firs two pictures, this one is characterized by much more mid-range hip and knee flexion angles. This allows a more optimal positioning of the COG over the front skate, while also positioning the body for a strong propulsive stride. In the picture below, I’ve put the three pictures side-by-side, with a box that encompasses the shoulders and the pelvis to provide a crude illustration of where the bodies weight is positioned. Note that the first box is shifted forward, and the second box shifted backward relative to the more optimal stride position.
With all of that said, the criterion for an optimal position is relatively similar for most skaters, but the outcome will be much different based on individual structural differences. As I noted above, an individual with longer femurs and a shorter torso may look a little more like the first picture in order to keep their weight positioned appropriately. An individual suffering from femoroacetabular impingement will have limited hip flexion ROM (typically around 90 degrees, compared to 120+) and will therefore need to maintain a slightly higher skating position to minimize stress to their anterior-superior hip labrum (the most common site of tears), and their anterior hip capsule. The point here is that optimal will look different for everyone, and it’s important to identify WHAT exactly may be limiting an individual’s ability to skate at a lower depth (if they appear too high, which is the most common complaint). It could be strength, positional awareness, or structure, all of which are trainable/coachable, but they require very different strategies to address.
2) When you say that most skaters with shorter, choppier strides are “naturally tighter”, what does this mean exactly? Is there any point in working with a skater that fits into this category to attempt to develop the flexibility and ROM necessary to have a closer to ideal knee and hip flexion?
This is an observation I’ve noticed from my time as a player and as a strength and conditioning coach. Stiffer players tend to be faster. This is true in almost all sports. They tend to be higher force output individuals, probably because the stiffness allows them to transfer energy and reduce force better. Stiffness, by definition, means it takes more force to displace the joint through any given range of motion; it doesn’t mean they can’t achieve full ROM. Although this is sometimes the case; the key is to know what they need and ensure that every player has that plus a little “wiggle room”. The idea that more flexibility is better is drastically misguided, and stiffness gets a really bad reputation when it probably shouldn’t.
3) You wrote that about 45-degrees is an optimal stride angle. I’ve noticed that for really effortless looking skaters who have green knee bend and hip flexion it sometimes seems like they are pushing almost straight out to the side at times. I know that just doesn’t sound right and I’m sure there’s no way the mechanics can work but maybe there’s a radius / arcing motion at play that makes it look that way. Just curious if you have ever studied that?
The 45-degree angle is optimal simply because of physics; think Newton’s laws. When an individual pushes through the ice, the stride leg is creating the propulsive force and the glide leg is determining the direction the individual will move, within reason. If a players stands with both skates pointing straight ahead, and pushes straight to the side with the right skate, he/she will either: A) Shave ice with their left skate or B) Fall over. This is despite the “glide leg” being oriented straight ahead. The vector that the individual pushes at will strong bias their movement in that same direction. Just as a push straight to the side would push them straight sideways, a push straight back would push them straight forward. This latter scenario would be ideal, but given the contour of the skating blade, they wouldn’t gain any friction. 45 degrees (or some slight variation of it) maximizes the combination of the forward propulsion vector AND skate blade contact.
That’s a wrap for today. If you haven’t yet downloaded your copy of Breakaway Hockey Speed, you can do so for FREE by entering your name and email in the form below!
Please enter your first name and email below to sign up for my FREE Athletic Development and Hockey Training Newsletter!
Managing Structural and Functional Asymmetries in Ice Hockey: Part 2
Part 1 of this series described anatomical asymmetries that all humans have, and how they can lead to predictable patterns and functional asymmetries. Part 2, below, will dive into how these patterns directly affect hockey performance and how they may contribute to common hockey injuries.
Influence on Hockey Performance
These positions are not inherently harmful. In fact, everyone should possess the ability to get into and out of these positions, bilaterally. Problems arise when an athlete gets stuck in a pattern and is unable to achieve the reciprocal position. This causes a shift in neutrality and increases the likelihood the athlete will need to push past joint end-range to achieve a functional outcome. Specific to skating in hockey:
A left hip positioned in a state of external rotation and abduction will make it more likely that the athlete will drive through end rage to achieve the desired stride length, which can cause compensatory SI joint stress and/or movement in forward skating.
A left hip positioned in a state of flexion will make it difficult to recover the leg fully under the body without standing up higher, which may cause some players to recover this leg slightly outside of their hips.
During crossover strides to the left, the left hip will be unable to adduct and drive under the right leg, a huge source of power.
During crossover strides to the right, the right hip will be more likely to drive through end range internal rotation and adduction, which can also cause a resultant gapping stress to the right SI joint.
Application to Common Hockey Injuries
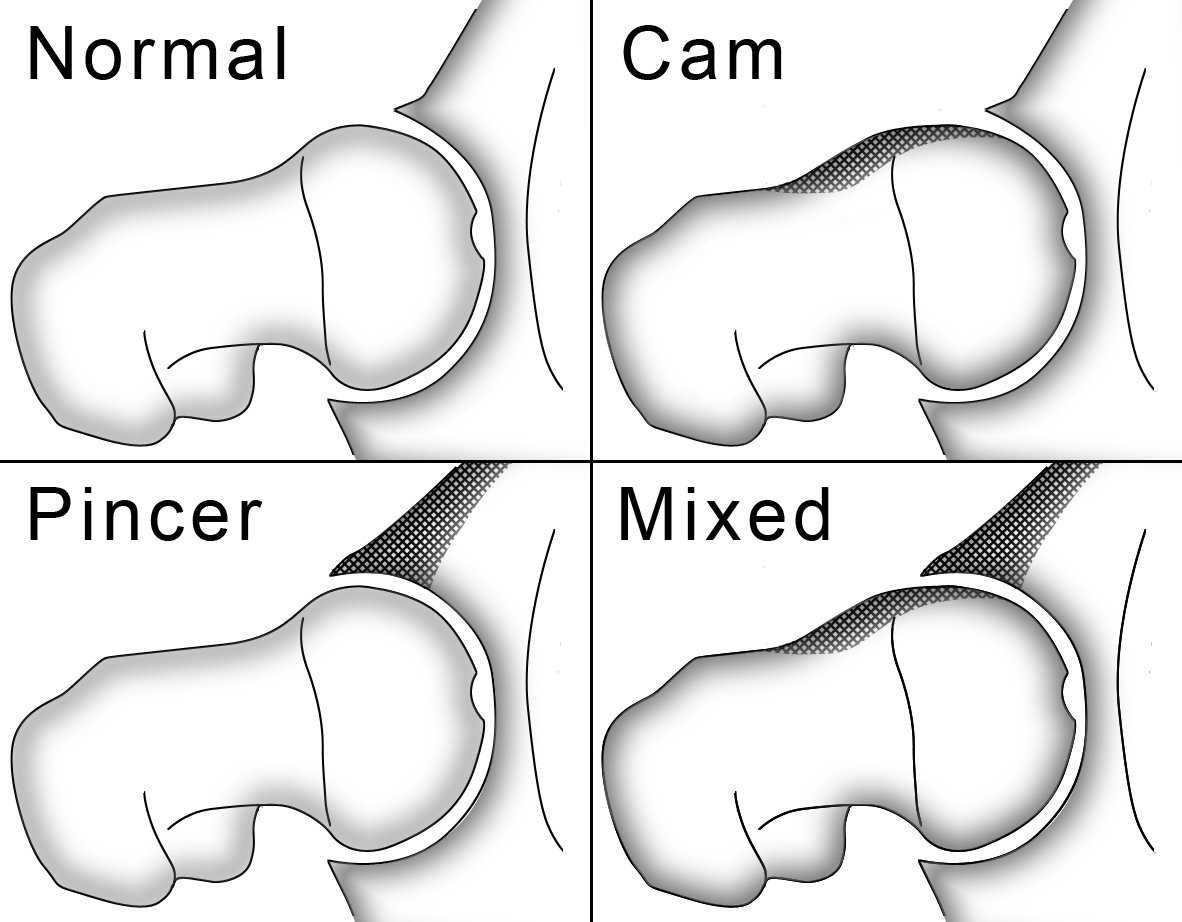
Interestingly, femoroacetabular impingement (FAI) which affects the overwhelming majority of elite level hockey players involves a loss of hip flexion, adduction, and internal rotation. While the two types of FAI, CAM and pincer, differ in the site of bony overgrowth, it’s clear that these injuries can become worse over time as players continue to push through joint end range and force bone on bone contact. Referring to the list above, it’s apparent that a left hip positioned in a state of flexion will increase the probability that a player will drive through end range hip flexion on that side; likewise, a right hip positioned in adduction and internal rotation provides a mechanism for excessive bony contact on that side. In other words, this same pattern provides a mechanism through which hockey players can develop FAI on both sides.
Similarly, because the left hip is positioned in a state of external rotation and abduction, the adductors are positioned long. As the stride leg is extended, these adductors are forced to decelerate the leg near their end-range, making it more likely that these muscles will become overstretched/strained and tear. In addition to the compensatory SI joint movement that the forward stride can create on the left side, driving through end-range external rotation can also cause a forward migration of the femoral head within the joint, causing excessive strain and laxity across the anterior hip capsule. Both adductor strain and anterior hip capsule laxity are common causes of “groin pain” in hockey players. Laxity in the capsule also allows for excessive accessory motion within the joint, which can cause labral damage and eventual osteoarthritis.
On the opposite side, the right adductors are positioned short and can become extremely dense and fibrotic. The predominant thought currently is that sports hernias are caused in large part because of a tug of war across the pubic symphysis between dense adductors and weak abdominals. The adductors progressively win this battle in an erosion-like fashion, which causes a fraying of the structures in the area of the superior surface of the pubic bone. Not surprisingly, sports hernias are more commonly found on the right side.
Naturally, early recognition is key. Indeed, while not every hockey player I’ve tested falls into one of PRI’s patterns, every hockey player with a history of hip injuries that I’ve tested does.
Subjectively, players may report having a more difficult time turning or crossing over to one side compared to the other. Similarly, they may have a preference for or feel more explosive when stopping and/or pivoting on one side compared to the other. While structure clearly influences function, function similarly influences structure. Simply, as players bias toward a certain position or pattern, all of their body’s systems, most notably their nervous and musculoskeletal systems, will adapt to the stresses. Often times, a small bias can snowball into a glaring asymmetry later down the road. This process may take years to develop, but can have dire consequences on a player’s health, performance, and career longevity.
Superimposed Occupational Biases
The discussion on structural and functional asymmetries is further complicated by occupational biases. In this sense, “occupation” simply refers to the asymmetrical patterns that players of different handedness and positions perform regularly throughout their seasons. For example, a right-handed player will likely perform THOUSANDS of high velocity, high power rotations toward the left (think slap shot) that they will not perform toward the right during a season. A goalie will likely bias toward a side-bent positioned on his stick side. These occupational tendencies are superimposed upon the asymmetries discussed above, and can help alleviate or further exacerbate some of the aforementioned consequences.
Wrapping Up
In addressing these issues, it’s necessary to keep the player’s injury history, current structural and functional presentation, and current and future occupational demands in mind. Often times, it is wise address asymmetries secondary to a loss of joint neutrality first, as it is impossible for muscles to function optimally if they are positioned poorly. Using repositioning techniques from PRI, typically breath-driven exercises involving asymmetrical targeting of specific muscles, can help restore and reinforce neutrality, and interrupt a downward spiral of compensatory adaptations. The off-season is an appropriate time to assess players for these imbalances, and to increase the volume of strategically asymmetrical exercises. Players should be monitored periodically throughout the season to help minimize the cumulative damage a season of play from a non-neutral position can create. Ultimately, following this approach can help fend off many of the acute, progressive, and chronic non-contact injuries players face throughout their careers.
To your success,
Kevin Neeld
Please enter your first name and email below to sign up for my FREE Athletic Development and Hockey Training Newsletter!
Limitations to Optimal Skating Performance
I wanted to kick this week off by following up on an article from last week on a few tips to help hockey players improve their skating technique. If you missed it, you can check it out here: 3 Keys to Developing Optimal Skating Technique
In that article, I alluded to the fact that players often have limitations that aren’t purely a failure to express their full capacity. In other words, they can’t simply be “cued” into skating better, they have some other issue that needs to be addressed to either remove a barrier to optimal performance or improve their capacity for optimal performance.
Barriers to Optimal Skating Depth Achieving an optimal skating depth is important for maximize stride length/power, as well as stability and resilience to unexpected contact or obstacles. That said, there is a significant number of players that don’t skate lower because they flat-out cannot get there. The two most common culprits are:
Femoroacetabular Impingement (FAI)
A lack of strength
Of these two limitations, FAI is structural and typically affects older more advanced players that have put a lot more mileage on their bodies, whereas a lack of strength is more functional and can affect players at all levels but typically affects younger players.
I’ve written a lot about FAI on the past (See: Training Around FAI; Performance Training: Adaptations for FAI; and An Updated Look at FAI), so I’ll keep it simple here, but the idea is that there is a BONY limitation to hip flexion range of motion. In other words, the player cannot and never will be able to achieve a deeper skating stance (without surgery) and attempting to force a lower depth, or even spending significant amount of time near end-range will almost definitely shred the labrum. In these cases, the players essentially have two options: 1) Get surgery; 2) Skate slightly higher. Given that these limitations tend to be cumulative over time, I wouldn’t be quick to jump to surgery unless the player is noticing significant symptoms. There are a ton of players competing at the highest levels in the world that are simply working around these limitations. That said, it’s still important to be aware of them, so you don’t attempt to “drive through” them on or off the ice.
A lack of strength is one of the most common issues we see in youth players who cannot achieve or maintain a deep skating stance. This is pretty straight-forward; they can’t skate in a deep position because they don’t possess the strength to hold themselves there. Hopefully the coaches reading this will understand the difference between “choosing not to” and “not possessing the capacity to do so”. One, the former, may justify some enthusiastic reminders to get into a deeper stance; another, the latter, involves a different approach. At youth levels (squirts through bantams), you’re likely to see a lot of the latter, meaning you can save yourself some throat irritation and mental anguish by just training the kids to improve their strength off the ice, instead of yelling at them on the ice.
If you lack equipment, as in most youth settings, an easy way to do this is with what I call “IsoHolds”. We generally do these in two positions: Squat IsoHolds and Split Squat IsoHolds. Split Squat IsoHolds are a more advanced variation, as they require single-leg strength, but ultimately I think this is the more advantageous option because of the benefits of single-leg training as well as the improvements in flexibility of the back leg. A Squat IsoHold is essentially a “Wall Sit” without the wall. I haven’t had an athlete do a Wall Sit in over 10 years; I stopped once I realized that the athlete did very little to hold the wall up, but the wall did a lot to hold the athlete up. It’s interesting how few youth players can even achieve a quality squat position, let alone hold it for prolonged periods of time (e.g. 30s). Most start the full body quiver around 20s, but few even get there since the form/technique breaks down before then. For other benefits of IsoHold work, check out this video:
Barriers to Optimal Power Transfer
Achieving an optimal skating depth and full stride length (including the toe flick, as I mentioned in the previous article) will help ensure optimal power generation with each stride. Ultimately, however, skating speed is dependent upon both optimal power generation AND optimal power transfer to the stance leg. This is the old shooting a cannon out of a canoe analogy. It doesn’t matter how explosive the cannon is if it’s stationed on an unstable base. More relevant to hockey, the most common “energy leaks” I see in players involve poor positioning and stability at the foot, hip, and lumbar spine (lower back).
Foot Stability The foot is often an overlooked piece of the puzzle in hockey players because it’s locked away in a hard boot. That said, the foot is incredibly important in maintaining stability of the skate, as it’s the final link between the body and the blade. I’ve learned a lot from Jim Snider, the Strength and Conditioning Coach at the University of Wisconsin, over the last several years, but when he told me that players that have collapsed arches in their feet (or, quite differently, arches that collapse) tend to ride their inside edges a big light bulb went off for me. The bottom line is that over-pronation of the foot on the glide leg translates into a mild collapse of the skate blade toward the inside edge. This increases the friction of the skate on the ice, decreases glide efficiency and ultimately dampens the power generated from the opposing leg.
An inward collapse of the foot also tends to cause an inward collapse of the knee, which can cause problems higher up. Just because the foot is locked into a skate boot doesn’t mean it’s not important. At Endeavor, we’re constantly looking at how our players’ feet position and respond to loading off the ice, and try to sift out which players have collapsed arches (which are typically better candidates for orthotics) and which have arches that collapse (which can typically be trained back to optimal function).
Hip Stability Just as an inward collapse of the foot can cause an inward collapse of the knee, poor hip stability can cause the femur (and knee) to collapse inward too. In other words, these stability issues travel both ways, from the foot up and from the hip down, and can have similar consequences. When the knees collapse in, it can cause a player to ride the inside edge on their glide leg, but it can also limit the power capacity of the stride leg. It’s a double-edge sword. David Lasnier filmed a video demonstrating this inward collapse during a Box Jump. Can you see it?
This is EXTREMELY common in female athletes and in younger athletes in general, and provides another great example of how off-ice training can transfer to on-ice improvements. Because this collapse is evident in a lot of off-ice exercises (almost every double- and single-leg jumping or strength training exercise), we have ample opportunity to improve this pattern off the ice. In the case of the box jump, the high levels of power generated by the hips are being transferred down to the ground through a wobbly base (which also limits power production of the muscles that attach to the knee, such as the quads, hamstrings, and gastrocnemius, one of the “calves”). You can address this by both cuing the athlete into more optimal alignment and by including exercises to improve their hip stability such as glute bridges, lateral miniband walks, and backward monster walks.
Lumbar Stability While skating, it’s important for players to maintain a neutral lumbar spine position, meaning a slight inward curve. As with sprinting off the ice, maximal speed on the ice utilizes diagonal force transfer between your glutes and opposite lats (or hip and opposite shoulder).
Note how the left “Lat” in red has fibers that appear to connect almost directly into the right gluteus maximus.
As one hip flexes, so does the opposite shoulder (stretching this lat-glute connection); at the same time, as one hip extends, so does the opposite shoulder (shortening this lat-glute connection). This connection provides an incredible opportunity for force transfer between the upper and lower body. Maximizing force transfer is predicated upon maintaining the transitional segments (e.g. the lumbar spine) in an optimal position, neutral, to do so. While I’ve seen hockey players that err both ways (too much extension and too much flexion), the majority tend to round excessively through their lower back (excessive flexion). This not only dampens efficient force transfer between the upper and lower body, it also can be a source of pain in itself. Know a hockey player with low back pain? This could be a reason why.
Once again, this is a positioning/movement fault that can be aggressively trained off the ice. It’s important for players to learn what “neutral spine” is and feels like, possess the ability to maintain it under load, and be able to transfer it to the skating position. Without question, every player is going to flex and extend through their lumbar spine during the course of every practice and every game. The goal here is to help them find a neutral position and make this their norm, so they don’t constantly gravitate or bias toward an excessively flexed position. One way to help bridge the gap between traditional off-ice exercises and on-ice work is through the use of slideboards. When a player is on a slideboard, you can help them find their optimal skating depth and a neutral lumbar spine position and see how they respond with a movement similar to skating and with fatigue.
Split Squat IsoHold into Slideboard
Note how Jeff Buvinow, who recently wrapped up a great 4-year career at Brown University, maintains a good skating posture and neutral spine throughout the exercise on the first slideboard. This video was taken the first time these guys had been introduced to this type of training, so the first day was a little sloppy, but they improved significantly over the next few weeks.
Wrap Up There is a lot to consider in maximizing skating performance, which is a positive. It means there are lots of areas for potential improvement. The players and coaches that have this information are better prepared to address all components of skating performance, including technical, structural, and functional factors. Not every player has the same potential, but the player who maximizes a lesser potential has an opportunity to out play the player that fails to maximize a greater potential.
Please enter your first name and email below to sign up for my FREE Athletic Development and Hockey Training Newsletter!
Get Ultimate Hockey Training Now!
“…an extremely rare comprehensive look at the present state of ice hockey training.”
“…a must-have for coaches and strength professionals at all levels of hockey.”
Hockey Training Radio Week: Part 1
This is an exceptionally busy week for me. On Thursday I fly up to Boston for a 3-day course, then immediately drive to Lake Placid to help with the end of the US Women’s National Team camp, before ultimately heading to Burlington, VT with the team for the IIHF World Championships. In a nutshell, I’ll be on the road from March 29-April 15th, which means I have 3 days to prepare for being gone for 2.5 weeks! That said, I’m pumped up for the course coming up and to spend some time with my friend Devan McConnell, who took over this year as the Head Strength and Conditioning Coach at UMass Lowell. I’m honored to have an opportunity to be involved with the US program as well, and humbled to work alongside such a great staff and group of players. Should be an exciting few weeks!
With all that in mind, I’m going to do my best to continue posting some hockey training and player development articles/videos for you over the ensuing weeks, but I’m really not sure how much down time I’ll have. Instead of leaving you stranded this week, I wanted to share a few interviews that I’ve done over the last month, starting with one I did with my friend Maria Mountain on Femoroacetabular Impingement (FAI). If you’re unfamiliar with FAI, this is one of the most common injuries that affects elite level hockey players currently and early intervention is key to minimizing the damage (e.g. those working in youth hockey should be aware of some of the potential developmental causes and symptoms). You can listen to and/or download the interview at the link below.
Enjoy! And if you have questions about any of the topics we talk about, please post them below.
To your success,
Kevin Neeld
P.S. As always, I appreciate you forwarding this along to anyone you think will benefit from the info! You can use the social media dropdown menu at the top right hand corner to share it via Twitter and Facebook!
Please enter your first name and email below to sign up for my FREE Athletic Development and Hockey Training Newsletter!










 Use CODE: "Neeld15" to save 15%
Use CODE: "Neeld15" to save 15%